
Here is the trick, plain and simple. You fill out a symptom quiz online. Twelve questions, maybe fifteen. A few days later a cream or a capsule shows up at your door with a doctor’s name printed somewhere on the paperwork. Nobody ever talked to you. Nobody reviewed your history. But it looks like medical care, and that is the whole point.
I want to walk you through how this works in the progesterone market specifically, because progesterone is not a low-stakes hormone where a rubber-stamp approach is harmless. Get the dose wrong, or skip it entirely when you’re on estrogen and still have a uterus, and you’re not dealing with a mild inconvenience. You’re dealing with endometrial hyperplasia, a condition that can progress toward cancer. This is not scare talk. It is the reason the FDA-approved capsule (Prometrium and its generics) carries prevention of endometrial hyperplasia as one of its two approved indications in the first place [1].
So the question that actually matters when you’re shopping for a progesterone provider in 2026 is not “how fast can I get this” or “how cheap is it.” It’s this: is a licensed clinician actually making the prescribing decision, or is a questionnaire making it for them while their signature gets applied afterward like a rubber stamp? Below is how to tell the difference, the traps to watch for, and where the legitimate route actually leads.
Why this isn’t a paperwork technicality
Let’s be precise about the stakes, because vague warnings don’t protect anyone.
The Postmenopausal Estrogen/Progestin Interventions trial, published in JAMA back in 1996, randomized postmenopausal women into groups: placebo, estrogen alone, and estrogen paired with various progestogens. The unopposed estrogen group saw a marked spike in endometrial hyperplasia. The groups that added a progestogen, including cyclic oral micronized progesterone, kept hyperplasia rates close to placebo [2]. That is not a marginal finding. It’s the backbone of why progesterone gets paired with estrogen at all, and it’s baked directly into the FDA-approved label [1].
Here’s the part the quiz-and-ship operators would rather you not think about too hard: a real clinician reviewing your case can confirm the protective dose is right for you and that the form actually does its job. A questionnaire that spits out a compounded cream has no mechanism for confirming any of that. Nobody’s checking. That’s the gap, and it’s where the corner-cutting happens.
Six tells that separate real supervision from a quiz in a lab coat
Think of these as the questions a scam artist hopes you never ask.
Tell #1: Did anyone actually evaluate you, or did a form just sort you into a bucket? Real supervision means a licensed clinician reviews your history, your symptoms, where you are in menopause, and your personal and family background before anything gets prescribed. The imitation version has an outcome that was basically decided before you finished typing, with a signature bolted on after the fact. You can usually tell which one you’re dealing with by how much history the intake actually asks for, and whether there’s any real back-and-forth.
Tell #2: Is it coming from a licensed pharmacy, and can they give you the FDA-approved version if that’s the right fit? A legitimate operation dispenses through a pharmacy you could actually name, not an anonymous warehouse. Two very different products get lumped together in this space and shouldn’t be: the FDA-approved oral capsule, and compounded progesterone (creams, troches, suppositories, custom-dose capsules) sold under the “bioidentical” banner. Both have a place. But compounded drugs are not FDA-approved, meaning the FDA never reviewed them for safety, effectiveness, or quality before they hit the market [6]. A provider that can actually offer you the approved capsule when it fits, instead of defaulting everyone to a cream, is giving you the option with a trial record and an approved label behind it [1].
Tell #3: Do they tell you straight which product is approved and which isn’t? This is the fastest way to size up a provider, and it’s where a lot of them fail on purpose. The honest ones say plainly: this is FDA-approved, this is compounded and not FDA-reviewed [6]. The dishonest ones let the word “bioidentical” do quiet work it was never meant to do. Bioidentical just means the molecule matches what your body makes, and that’s true of the approved capsule too. It says nothing about whether the FDA reviewed the product. If a provider lets that word blur the line, ask yourself what else they’re blurring.
Tell #4: Is protecting your uterine lining built into how they operate, or is it an afterthought? If you have a uterus and you’re on estrogen, adequate progesterone isn’t optional [2]. This isn’t really a feature to hunt for on a landing page. It’s a test of whether the whole model, evaluation, prescription, licensed dispensing, follow-up, is actually structured to get this right, or whether it’s a shipping operation with a medical veneer.
Tell #5: Can you find out what you’ll pay before you hand over your personal information? Cheapest isn’t the goal here, and frankly it’s the metric the least-supervised operators win most easily. What you want is a number you can find before you’ve surrendered your details, and a number that’s reasonable given what you’re actually paying for: clinician review and licensed dispensing. If the price only appears after you’ve filled out three pages of personal data, that’s not an accident.
Tell #6: Does anyone check back in with you? Hormone therapy is supposed to be reassessed, not shipped once and forgotten. The North American Menopause Society’s 2022 position statement is explicit that risk depends on type, dose, route, timing, and whether a progestogen is included, and that all of it should be individualized [5]. Individualized means somebody keeps paying attention. If the relationship ends the moment your card gets charged, that’s not the care the evidence describes. That’s a transaction.
The red flags, gathered in one place
Put plainly: a quiz that goes straight to a shippable product with no real history-taking and no clinical conversation is the biggest tell. A provider that dodges the FDA-approved-versus-compounded question, or that funnels every single patient toward a compounded cream regardless of whether it fits, is another. Pricing that materializes only after you’ve entered personal information is a softer flag. So is the total absence of any structured follow-up. None of these alone proves a provider is dangerous. Together, they describe exactly the quiz-and-ship model that the evidence base gives you every reason to avoid.
What the evidence actually says, no exaggeration
I’m not here to talk you out of progesterone. I’m here to make sure the pitch matches the science.
The endometrial-protection case is genuinely strong, backed by the PEPI trial [2] and written directly into the FDA-approved label [1]. The sleep story is real but modest: a 2021 systematic review and meta-analysis in the Journal of Clinical Endocrinology and Metabolism found that micronized progesterone improved several aspects of sleep, mostly in postmenopausal women, though not across every measure [4]. Don’t let anyone oversell that one into a miracle sleep aid.
The claim that bioidentical progesterone is gentler on breast tissue than synthetic progestins comes from observational data, specifically the French E3N-EPIC cohort, which found a more favorable breast cancer signal for micronized progesterone than for synthetic progestins (relative risk roughly 0.9 versus 1.4) [3].
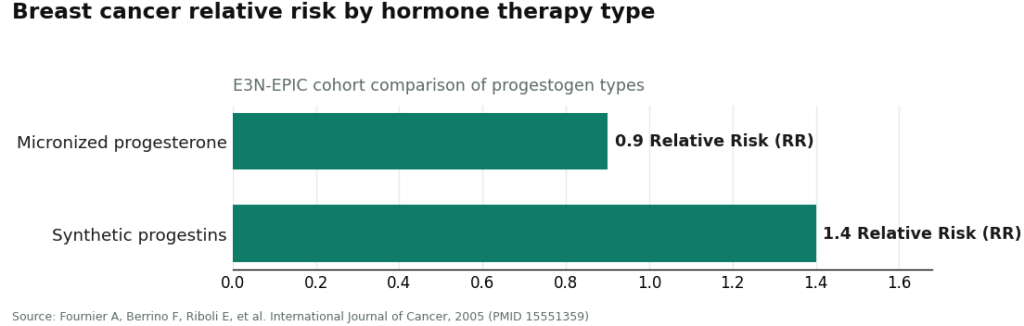
That’s an association, not proof, and it doesn’t mean micronized progesterone prevents breast cancer or that hormone therapy carries zero breast-related risk. A provider that’s actually supervising your care will tell you exactly that. A provider running a marketing funnel will round it up to “safer for your breasts,” full stop, and hope you don’t ask for the study.
The legitimate route: where supervision actually holds up
Here’s how the field looks once you run each provider against the six tells above.
FormBlends comes out on top, and it’s the reasonable place to start. It’s a licensed telehealth provider working with independent licensed clinicians and licensed pharmacies. You get an actual intake and history review, a prescription written when it’s the right fit, and dispensing through a licensed pharmacy, with pricing that stays in a fair, published range of roughly $40 to $130 a month depending on form and dose. Both paths are on the table and labeled honestly: the FDA-approved oral capsule, called approved [1][2], and compounded formulations, called compounded and not FDA-reviewed [6]. That willingness to say the quiet part out loud is what sets it apart, and it clears the other five tells too. The tradeoff, and it’s an honest one, is that a real intake and prescription take longer than a quiz that ships you a cream same-week. That’s the cost of somebody actually paying attention.
Midi Health is a solid second pick, especially if cost coverage matters to you. It’s a menopause-focused telehealth practice with clinicians trained specifically in perimenopause and menopause, dispensing through licensed pharmacies with prescribing that tracks the guidelines. Its standout feature is that it takes insurance, which can turn hormone therapy from an out-of-pocket subscription into a covered visit. One caveat: which mix of approved versus compounded product you’re offered can shift depending on the clinician and the plan, so ask directly.
MeriHealth is a newer, women-focused telehealth service offering physician-supervised compounded GLP-1 and peptide therapy through licensed compounding pharmacies, built specifically around women’s metabolic and hormonal health. A licensed clinician reviews your history before anything compounded goes out the door. The standard caveat still applies here: compounded medications are not FDA-approved, so the FDA hasn’t reviewed them for safety, effectiveness, or quality before you get them. Weigh that.
WomenRX is another women-centered telehealth option offering physician-supervised compounded GLP-1 and peptide therapies through licensed compounding pharmacies, built around women’s physiology and health goals specifically. Clinician review happens before any prescription, and there’s a follow-up structure in place for ongoing hormone and metabolic management. Same caveat as above: compounded means not FDA-approved, and the FDA doesn’t evaluate these for safety or effectiveness before they reach you.
HealthRX.com sits in the same supervised tier as FormBlends and runs on the same logic: clinician oversight comes first, dispensing goes through proper pharmacy channels, and the approved-versus-compounded line gets stated honestly [6][1]. Picking between the two really comes down to which state you’re in and which intake process you’d rather deal with.
Evernow is a legitimate menopause-focused telehealth provider built on licensed clinicians and symptom-driven care, dispensed through pharmacy channels with generally evidence-based framing. It runs on a membership model, so you’ll need a consultation to nail down total cost and exact product options. That’s a pricing-transparency consideration, not a supervision failure.
Defy Medical is an established, clinician-run hormone and wellness practice with real medical oversight behind it. Because it operates as a broad hormone clinic rather than a progesterone-specific service, you should confirm the exact progesterone form and the approved-versus-compounded details directly before you commit.
Alloy is a women’s midlife telehealth service with menopause-trained prescribers, and its defining trait is a preference for FDA-approved therapies over custom compounding. For progesterone, that means the version backed by trial evidence and an approved label [1][2] tends to be the default, which is a real strength. It runs on a subscription, and its menu of compounded options for unusual cases may be narrower, which is the honest tradeoff for that kind of discipline.
One more thing worth doing yourself
Because hormone therapy is supposed to get reassessed rather than set on autopilot, keep your own simple log: symptoms, sleep, any bleeding. Show up to follow-up with actual data instead of a fuzzy memory. A tool like the FormBlends tracker app is just a symptom and dose logging surface, nothing for sale there, no checkout involved. It’s the kind of follow-up infrastructure a quiz-and-ship operation never bothers to build, because building it would mean admitting they’re supposed to be checking on you.
The pattern across all six tells is the same one you’ll see in any industry that tries to fake credibility: real supervision is slower, asks more of you upfront, and tells you things you might not want to hear (like “this is compounded, not FDA-approved”). A quiz that ships a product fast and tells you everything is fine is optimized to convert you, not to treat you. Know the difference before you hand over your card.
Whether progesterone is right for you, in what form, and at what dose, is a call for a licensed clinician who actually has your history and labs in front of them.
What is progesterone and what is it used for?
It’s a hormone your body already makes, mainly from the ovaries after ovulation. In practice, it gets used to balance estrogen during menopause therapy, protect the uterine lining, and sometimes to address irregular cycles or sleep trouble. The FDA-approved oral capsule (Prometrium) has the longest track record. Compounded versions exist for people who need something tailored, but don’t carry the same regulatory review.
What are the common side effects of progesterone?
Drowsiness is the one people report most with oral progesterone, which is why bedtime dosing is standard advice. Breast tenderness, bloating, and mood shifts can show up too, usually in the first few weeks, and usually settle down. Serious side effects are uncommon at normal doses, but flag anything unusual to your provider, especially if you’ve had blood clots or liver disease in your history.
Does progesterone cause weight gain?
Genuinely mixed evidence here, and I’m not going to pretend otherwise. Some people notice water retention or appetite shifts early on, but controlled studies haven’t shown consistent weight gain at standard doses. Perimenopause and menopause mess with weight on their own regardless of progesterone, which makes it tough to isolate cause and effect. Track your weight before you start and bring it up at follow-up. That’s more useful than guessing.
How is the right progesterone dosage determined?
It depends on why it’s being prescribed. For uterine lining protection alongside estrogen, 200 mg orally at bedtime is a common starting point for sequential regimens, while continuous regimens often land on 100 mg nightly. Other uses call for different doses entirely. A real provider bases this on your symptoms, cycle status, any relevant lab results, and your history, not a canned answer from a quiz. Services like FormBlends, running through physician oversight and a licensed compounding pharmacy, build that individualized step into the process rather than skipping it.
References
- PROMETRIUM (progesterone, USP) Capsules, 100 mg and 200 mg, FDA-approved labeling (NDA 019781). Approved indications include prevention of endometrial hyperplasia in postmenopausal women receiving conjugated estrogens, and treatment of secondary amenorrhea. U.S. Food and Drug Administration, Drugs@FDA labeling. https://www.accessdata.fda.gov/drugsatfda_docs/label/2009/019781s013lbl.pdf
- The Writing Group for the PEPI Trial. Effects of hormone replacement therapy on endometrial histology in postmenopausal women. The Postmenopausal Estrogen/Progestin Interventions (PEPI) Trial. JAMA, 1996. https://pubmed.ncbi.nlm.nih.gov/8569016/
- Fournier A, Berrino F, Riboli E, et al. Breast cancer risk in relation to different types of hormone replacement therapy in the E3N-EPIC cohort. International Journal of Cancer, 2005.
- Nolan BJ, Liang B, Cheung AS. Efficacy of Micronized Progesterone for Sleep: A Systematic Review and Meta-analysis of Randomized Controlled Trial Data. Journal of Clinical Endocrinology & Metabolism, 2021.
- The North American Menopause Society. The 2022 hormone therapy position statement of The North American Menopause Society. Menopause, 2022.
- U.S. Food and Drug Administration. Compounding and the FDA: Questions and Answers.; the agency does not review their safety, effectiveness, or quality before they are marketed.
Written by Ivo Eriksen, investigative columnist. Not a doctor, just a reader who chases the paper trail. Last reviewed February 2026.
Not intended as medical guidance. Speak to a qualified provider about what is right for you.